The Ross Procedure is a specialized cardiac surgery technique primarily used to treat aortic valve disease. The Ross Procedure involves the transplantation of a patient's own pulmonary valve (known as an autograft) to replace a diseased aortic valve. A donated human pulmonary valve (known as a homograft or allograft) is then used to replace the patient’s removed pulmonary valve. This procedure has benefits including long-lasting durability and a survival rate comparable to that of individuals in the general population of the same age and gender, making it a valuable option for select patients with aortic valve disease.1,2
Ross Procedure Overview
History: Dr. Donald Ross, an accomplished surgeon in London, was a pioneer of aortic valve replacement using an allograft. This later evolved into what we now call the Ross Procedure. The procedure was first performed in 1967.
Patient Eligibility: The Ross Procedure is typically considered for young or middle-aged adults, particularly those with aortic valve disease, who are seeking a long-term solution that avoids the need for lifelong anticoagulant therapy (blood-thinning medication). This procedure is less commonly performed on elderly patients or those with specific contraindications.2,3
How the Ross Procedure Works2,4
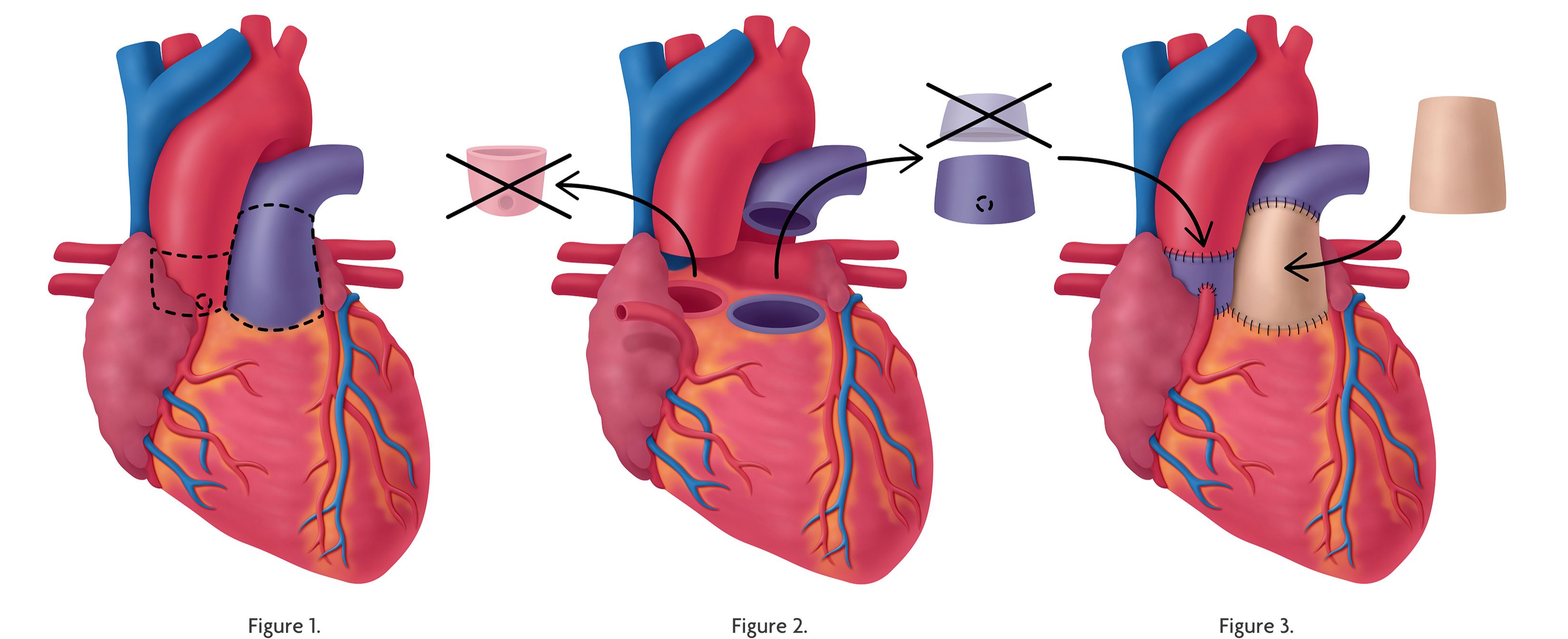
Figure 2. The patient’s diseased aortic valve is removed. Then the patient’s pulmonary valve is removed and resized to match the aortic valve position.
Figure 3. The patient’s pulmonary valve is moved to the aortic position. Then a pulmonary allograft is placed in the pulmonary position.
Excision of diseased aortic valve: The surgeon first removes the diseased aortic valve.
Autograft: The surgeon removes the patient’s pulmonary valve, which is located between the right ventricle and the pulmonary artery. This valve, known as a pulmonary autograft, is then sized to match the aortic valve position, taking care to preserve the pulmonary valve within the graft.
Allograft: To replace the removed pulmonary valve, a donated human pulmonary valve (known as a pulmonary homograft/allograft) is used. This is obtained from a deceased tissue donor.
Transplantation: The pulmonary valve autograft is placed in the aortic position to function as the new aortic valve. The pulmonary valve homograft/allograft is then implanted in the pulmonary position to replace the removed pulmonary valve.
Recovery and Follow-Up: After the procedure, patients undergo a period of recovery and rehabilitation, including close monitoring of their heart function. Regular follow-up with a cardiologist is essential to assess valve function and overall heart health.
Advantages
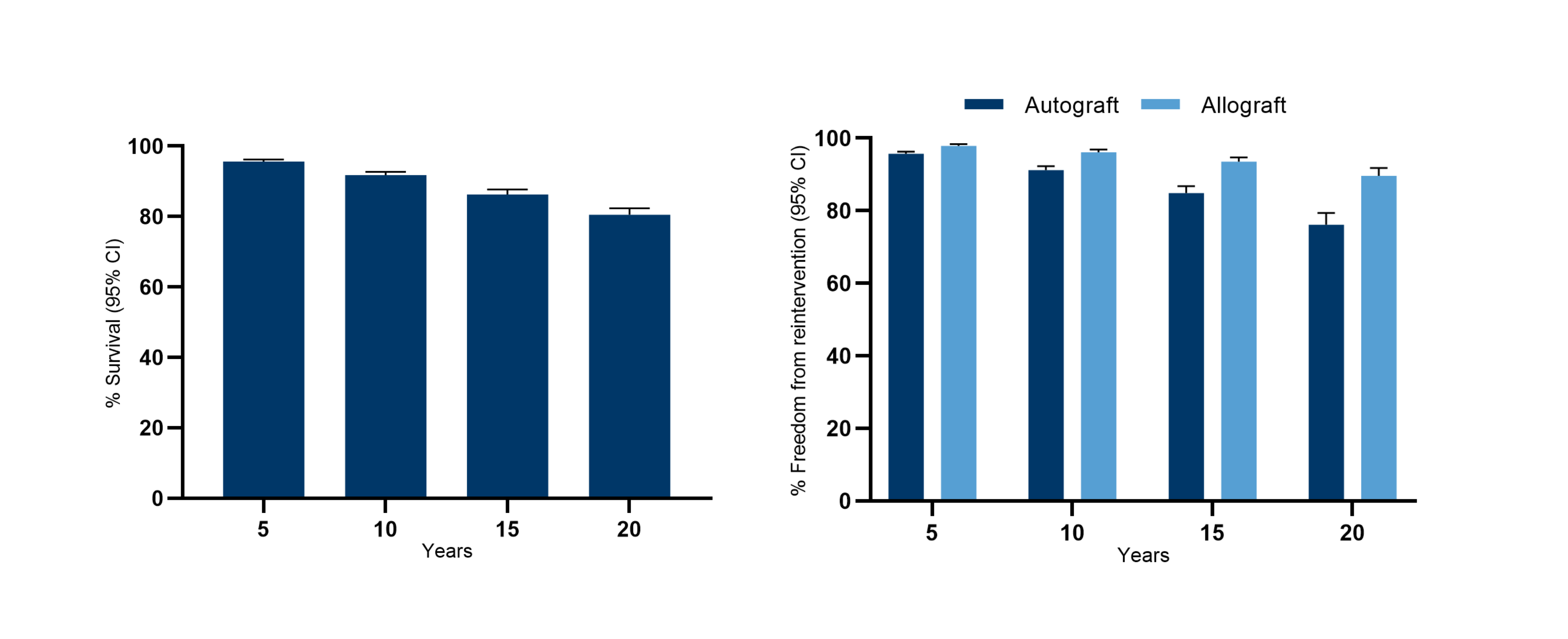
- Low Risk of Valve Degeneration: The Ross Procedure offers excellent long-term durability for both the pulmonary and aortic valves.2,5 While the aortic valve is under high pressure, the pulmonary valve is at a lower pressure. The patient’s own tissue will better adapt to and withstand the high-pressure environment versus other valve options. This reduces the likelihood of valve degeneration and the need for future valve replacement surgeries.
- Improved Hemodynamics: The use of a patient's own tissue often leads to improved long-term hemodynamic performance, both at rest and during exercise, with transaortic gradients comparable to those in healthy individuals.2
- Avoidance of Lifelong Anticoagulants: Unlike mechanical or bioprosthetic valve replacements, which require potentially lifelong anticoagulant therapy, the Ross Procedure allows patients to avoid blood-thinning medications, which correspondingly reduces the risk of thromboembolic events,2 making it an attractive option for younger individuals.
Considerations and Limitations
The Ross Procedure is a complex surgery that requires a highly skilled cardiac surgeon. It may not be suitable for all patients, especially those with specific medical conditions or older individuals. The decision to undergo this procedure should be made in consultation with a cardiac surgeon and healthcare team.
Additional Resources:
CardioGraft® Pulmonary Valve Product Specifications
Webinar | The Ross Procedure: Clinical Overview, Surgical Outcomes, and Patient Outcomes
Ross Procedure Clinical Outcomes
References:
- Flynn CD, De Bono JH, Muston B, Rattan N, Tian DH, Larobina M, O’Keefe M, Skillington P. Systematic review and meta-analysis of long-term outcomes in adults undergoing the Ross procedure. Ann Cardiothorac Surg. 2021 Jul;10(4):411-419. doi: 10.21037/acs-2021-rp-30.
- Mazine A, El-Hamamsy I, Verma S, et al. Ross Procedure in Adults for Cardiologists and Cardiac Surgeons: JACC State-of-the-Art Review. J Am Coll Cardiol. 2018;72(22):2761-2777. doi:10.1016/j.jacc.2018.08.2200
- Sibilio S, Koziarz A, Belley-Côté EP, et al. Outcomes after Ross procedure in adult patients: A meta-analysis and microsimulation. J Card Surg. 2019;34(5):285-292. doi:10.1111/jocs.14020
- Brown KN, Kanmanthareddy A. Ross Procedure for Aortic Valve Replacement. [Updated 2023 Feb 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537249/
- Fricke TA, Skillington PD, Shi WY, et al. Pulmonary Valve Function Late After Ross Procedure in 443 Adult Patients. Ann Thorac Surg. 2020;109(4):1127-1131. doi:10.1016/j.athoracsur.2019.07.060